The process that every human being goes through to learn to eat and drink is incredibly complex. Eating and drinking (also referred to as “feeding” and “feeding development”) start in infancy and take several years for a child to master.
Further, feeding involves all areas of a child’s development: motor/movement, cognitive/thinking, communication and social-emotional skills.
When an area of development is not working to its fullest potential, challenges can arise for a child in their quest to feed and drink independently. Therefore, when supporting a child’s feeding development, it is critical to understand their specific needs and capacities and offer support that is in alignment with them. The earlier challenges can be identified, the sooner support can be provided, resulting in happier, healthier children and caregivers!
Feeding development is comprised of these 5 primary components:
1. Positioning
2. Swallowing
3. Sensory Systems
4. Food & Liquid Textures and Consistencies
5. Relationships
Positioning
Positioning refers to the way we hold a child in our arms or on our laps, and how we place a child in a chair, seat or on the floor for mealtimes. Ensuring a child is properly positioned during feedings is critical to keeping them safe. Additionally, when a child is well-positioned, they feel safer and ready to handle the task of learning to eat and drink!
There are 6 key elements of positioning for infants and children of all ages:
| Hips | Positioned at 90 degrees |
| Trunk | Upright, not leaning forward, backward or sideways |
| Shoulders | Level and facing forward |
| Head | Chin slightly tucked toward chest, head upright and facing forward |
| Knees | Positioned at 90 degrees |
| Feet | Supported on the floor, chair footrests or another object, flat position |
The way we position a child will depend on:
- Age of the child
- General developmental skills of the child, especially physical capabilities
- Individual needs of the child (i.e., higher elevation of body during feeding due to reflux, increased head/trunk support due to low muscle tone, etc.)
- Caregiver’s abilities
- Resources available in the environment

Swallowing
Proper swallowing helps with digestion and prevents food and liquid from going into the lungs, which can lead to serious health issues. Eating and drinking during mealtimes should be enjoyable for children and their caregivers. However, when swallowing challenges arise, feeding can sometimes become uncomfortable, scary and even life-threatening.
There are 4 phases of the swallow:
- Phase 1: Oral preparatory (a)
- Phase 2: Oral transit (b)
- Phase 3: Pharyngeal (c)
- Phase 4: Esophageal (d)
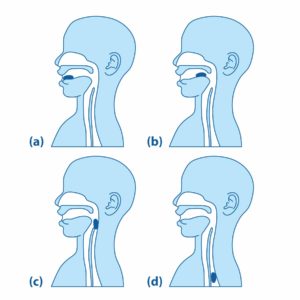
Each phase helps collect and transport food and liquid from the mouth through the throat and into the stomach.
Aspiration is when food or liquid passes into the airway and lungs instead of moving into the stomach where it belongs. Depending on the child (and how often and how much he aspirates), improper swallowing can lead to illness, malnutrition, dehydration and even death. If a child is suspected of aspirating, it is critical to contact medical professionals for support.
Swallowing Challenges
| Signs and Symptoms of Swallowing Challenges | Description (What It Looks Like) |
|---|---|
| Coughing or Choking | Child coughs or chokes during or after swallowing food or liquid |
| Gurgly, “Wet” Sounding Voice or Breathing | Child’s voice or breathing sounds wet during or after swallowing food or liquid |
| Complaints of Discomfort | Child experiences the sensation of food being stuck in the throat during, following and/or in between meals; reports pain or discomfort with eating/drinking, or food comes back up into the mouth after swallowing |
| Watery Eyes | Child’s eyes water during or after swallowing food or liquid |
| Change in Color | Child’s face changes color (pale, red or purple/blue) during or after swallowing food or liquid |
| Fever | Child experiences fever following a meal |
| Facial Grimace | Child displays uncomfortable faces during or following feedings |
| Change in Breathing | Child’s breathing becomes unusually fast or slow, child stops breathing while feeding, or child wheezes or gasps for air during or after swallowing food or liquid |
| Lung Infections | Child experiences infections in the lungs or airway |

Sensory Systems
The sensory system is a complex group of neurons (cells in the body), cell pathways and parts of the brain that work together to allow an individual to feel different sensations from the environment. Every individual has a sensory system that is unique to them. The way a child’s sensory system is made will impact the way he experiences the world, including feeding development. Eating is the most sensory-rich activity a child will experience!
The 8 Senses That Make Up Our Sensory Systems
| Sense | Description | Example |
|---|---|---|
| Seeing (Vision) | Information that comes to the body through the eyes (what one sees) | Bright lights, dim lights, colors, shapes, faces, fast- or slow-moving objects, distance to objects and faces (near or far), etc. |
| Hearing (Auditory) | Information that comes to the body through the ears (what one hears) | Loud and soft noises, voices, music, high- and low-pitched sounds, etc. |
| Smelling (Olfactory) | Information that comes to the body through the nose (what one smells) | Strong and light smells, unpleasant and pleasant smells, scents of people, places and foods/liquids, etc. |
| Tasting (Gustatory) | Information that comes to the body through the tongue (what one tastes, eats or drinks) | Different flavors (sweet, sour, salty, bitter, etc.) |
| Touching (Tactile) | Information that comes to the body through the skin and mouth (what one feels on the body) | Light touch, deep pressure touch, temperatures, pain, vibration, different textures (smooth, lumpy, crunchy, hard, etc.) |
| Balance and Movement (Vestibular) | Information that comes to the body through different movements (what one feels when the body moves up, down, backward, forward, sideways, rotationally, etc.) | Rocking, swaying, swinging, turning, bouncing, spinning, standing up, sitting down, balancing, etc. |
| Joints and Muscle Awareness (Proprioception) | Information that comes to the body through sensations felt in the joints and muscles (what one feels when their body is in different positions and in contact with objects, such as people, chairs or the ground) | Sitting, walking, running, crawling, climbing, stomping feet, jumping, clapping hands, pushing and pulling heavy items, lifting and carrying items, etc. |
| Recognizing Sensations Inside the Body (Interoception) | Information that comes from within the body and that relates to one’s physical state or condition (what one senses from the organs) | Hunger, thirst, fullness, heart rate, breathing rate, temperature, bowel and bladder needs, etc. |
Hyper- and Hyposensitivity
Some children have sensory systems that show increased (hypersensitivity) or reduced (hyposensitivity) sensitivity to certain sensations: for example, a child who covers their ears while in a noisy room, an infant who frequently falls asleep at the bottle or breast, the child who engages more in mealtimes following rocking and hugs, or the child who gags on new food textures. There are many reasons why a child might have a sensitive sensory system. Sometimes we can tease out the “why” and sometimes we may never uncover an answer. By being aware of what our children show us and noticing how they respond, we can make our best attempt at creating positive and manageable mealtime experiences that also grow their feeding capacities over time.

Check out additional parenting resources!
View our expanded list of recommended parenting websites, books and other resources organized by topic.
Food & Liquid Textures and Consistencies
From soft and smooth, to lumpy and bumpy, to crunchy and hard, to thin and thick – not all food and liquid feel the same or require similar skills to eat and drink! Because of this, it’s helpful for caregivers to understand these differences and identify which may be best suited for a child based on their specific needs and skills. Choosing the right texture and consistency for a child makes mealtimes safer, and more comfortable and enjoyable for everyone. When children can eat and drink safely and comfortably, they tend to eat and drink more!
Why might a child need a certain texture or consistency? Or why might a child not be able to have a certain food or liquid? There are many reasons why we might choose to offer certain foods and liquids and/or avoid offering others to a child. A medical provider who specializes in pediatric feeding can offer support in this area.
Some reasons include:
- Medical conditions involving reflux, the lungs or heart
- Children who are born early (prematurity)
- Structural/anatomical differences (i.e., cleft lip and/or palate)
- Neuromuscular disorders such as cerebral palsy
- Developmental disabilities such as Down Syndrome

Types of Textures
| Solid Food Textures | Description | Example of Foods |
|---|---|---|
| Pureed/Extremely Thick | Usually eaten with a utensil Cannot drink from a cup or straw Does not require chewing Smooth, no lumps Does not pour Falls off spoon in single spoonful and holds shape on plate/tray/table | Blended vegetables, fruits and meats, thick cereals |
| Minced and Moist | Can eat with utensil, chopsticks or sometimes hands Can be shaped and scooped on plate/tray/table Small lumps visible Lumps are easy to squish with tongue Moist and soft Minimal chewing is required Does not require biting | Finely minced meats, finely minced or mashed fruits, vegetables and fish, thick cereals with small lumps |
| Soft and Bite-Sized | Can eat with utensil, chopsticks or hands Soft, tender and moist bite-sized pieces Can be cut without a knife Can be mashed or broken down with utensil Chewing is required Does not require biting | Cooked-tender meats, flaky fish, mashed fruits, steamed or boiled vegetables, soft cheese and eggs, soaked breads that are “moist” to touch |
| Regular | Normal, everyday foods of varying textures (soft, hard, crunchy, fibrous, chewy, dry, stringy, crispy, crumbly, etc.) Includes mixed or dual consistencies (foods + liquids → soups and stews) Age-appropriate Developmentally appropriate based on skill level of child Chewing and biting may be required based on food texture | All meats, vegetables, fruits, cheese, eggs, breads |
Types of Consistencies
| Liquid Textures | Description | Example of Liquids |
|---|---|---|
| Thin | Fastest flowing liquid Flows like water Can drink from any nipple, cup, syringe or straw | Water |
| Slightly Thick | Slightly slower flowing than water Slightly thicker than water Can drink from any nipple, cup, syringe or straw | Breast milk, formula |
| Mildly Thick | Slower flowing than slightly thick liquids Thicker than slightly thick liquids Flows off of spoon quickly, but slower than thin liquids Can drink from spoons, most open cups and some closed cups and straws More effort required to drink from straw | Fruit nectars |
| Moderately Thick | Slower flowing than mildly thick liquids Thicker than mildly thick liquids Flows off of spoon slowly in dollops Can drink from spoons and open cups Smooth texture without lumps No chewing or processing required | Runny pureed fruits and rice cereals, sauces, gravies, honey |
| Extremely Thick/Puree | Slowest flowing liquid Thickest liquid Usually eaten with a utensil Cannot drink from cup or straw Does not require chewing Smooth, no lumps Does not pour Falls off spoon in single spoonful and holds shape on plate/tray/table | Blended vegetables, fruits and meats, thick cereals |

Relationships
Learning to eat and drink is relational! One of the primary ways a child learns how to take a bite, drink from a cup or taste a new food is through robust relationships and modeling (showing) of how to do these things by those around them. Early skills such as feeding must be learned. Additionally, learning new skills can be hard! This means that while children are developing, they need extra support from their caregivers to feel safe, stay calm and “try again!” Regulation, or a child’s ability to become and stay calm, is essential for development, especially for eating and self-feeding.
Learning to eat and drink is relational! One of the primary ways a child learns how to take a bite, drink from a cup or taste a new food is through the robust relationships and modeling of how to do these things by those around them.
Putting it All Together
So, as you can see, feeding is a much more intricate process than simply putting sustenance into our bodies. It is a foundational process for a child not only to thrive but to also learn and connect with their world. If you are having questions or concerns about your child’s eating and drinking development, connect with a medical provider, such as a pediatrician or a feeding specialist (speech-language pathologist or occupational therapist) in your area for additional support.
For more details on feeding best practices, download Holt International’s Feeding & Positioning Manual: Guidelines for Working With Babies and Children. In addition, check out the Ellyn Satter Institute for more useful feeding information.

Receive Family & Adoptee Support
All parents encounter challenges as their children grow up. And sometimes, issues may arise that leave you uncertain as to how best to respond. But not every issue requires therapy or counseling. The Holt Family & Adoptee Support program is here to help during those times.